Colic is a scary word to horse owners and veterinarians. However, some types of colic are much worse than other types. While 90% of colic cases resolve with minimal treatment on the farm, some require more intensive care. One such type of more serious colic is small intestinal strangulation, which is an obstruction of the blood supply and the lumen (the inside of the tube, where food passes through) of the small intestine.
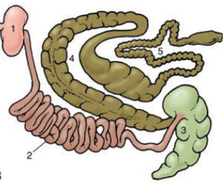
The horse’s gastrointestinal system is quite lengthy – it spans approximately 120 feet, and the majority (70-80 feet) of that is small intestine. Furthermore, it’s mostly floating freely in the abdomen, with minimal attachments to the body wall and surrounding organs. This conformation gives lots of opportunities for something to go wrong, whether that’s a twist, or some other way that the intestine ends up in the wrong spot.
The small intestine (or SI, for short) is the same in horses as it is in dogs, cats or humans. It’s made up of 3 segments – the duodenum, the jejunum and the ileum. The duodenum is the first section, just after it leaves the stomach and for about the next 12-16 inches (that’s it – so, not much goes wrong with the duodenum!) The jejunum makes up the bulk of the small intestine, and the ileum comprises the last foot or so before it enters the cecum. There are minor variations in these structures, but we don’t have to worry about them here. All this SI is suspended within the abdomen by a sheet of connective tissue called “mesentery”. (If you laid a garden hose straight across a towel, then picked the towel up at all 4 corners it would create the same effect.) The mesentery brings blood supply to the intestines.
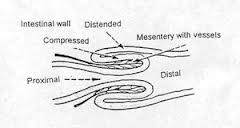
Small intestinal strangulation means that a section of SI is squeezed tightly – like wrapping a rubber band around your finger. This tight pressure cuts off both the blood supply as well as flow through the center of the “tube” of the SI. This process can occur a number of different ways, including masses, internal hernias, and intussusceptions (it’s a tough word, we’ll get to that). All of these are surgical problems, but there are various factors which contribute to outcome and prognosis. We’ll outline the most common strangulating lesions below.
Strangulating lipomas: One of the more common obstructions we see, especially in older horses, is something called a strangulating lipoma. A “lipoma” is a benign fatty tumor that develops within the mesentery. (We call it “benign” because it’s a tumor that does not metastasize to other parts of the body. But that doesn’t make it less serious.) Lipomas typically hang from a stalk, which makes them a ticking time bomb for colic – at some point in the horse’s life it can wrap itself around the small intestine, cutting off the blood supply and causing sudden, extreme signs of pain.

Internal hernias: A “hernia” is when normal tissue slips through a normal or abnormal hole in the body. When we talk about small intestinal herniation, we mean there is an opening that the small intestine moves through and gets trapped. These openings can be anatomical openings (such as an inguinal hernia) or holes that have developed in other structures due to previous trauma or a defect from birth (such as a tear in the mesentery or the diaphragm). A small, normal hole in the mesentery is called the “epiploic foramen”, which can occasionally trap the small intestine and cause a strangulation.
Intussusception: Prounounced in-tus-sus-sep-shun, these are more common in younger horses. This occurs when one piece of small intestine telescopes into another piece of small intestine. We often suspect that a heavy parasite burden leads to this disorder, however sometimes we just don’t find an answer. While this isn’t truly a “strangulation”, it kind of acts in a similar manner.
Regardless of how it happens, small intestinal strangulations are a serious problem. Horses are often in extreme pain and are found thrashing. They have elevated heart rates, oftentimes over 80 bpm and head wounds are not uncommon (from throwing themselves into the wall). The clinical signs of associated with this are not pretty. Further diagnostics can be done to confirm, such as a rectal exam and ultrasound, but referral to a surgical facility should be foremost on your mind.
Why is it so painful? Because the blood supply to the area of strangulated intestine has been cut off, and the tissue is in the process of dieing. While the tissue is compromised, it is releasing toxins into the bloodstream, which further sickens the patient. These cases become critical quickly and surgery is really the only option.
Once the horse goes to surgery, some questions still remain. (You can answer some of those questions at this blog.) The tissue is not always dead, and simply removing the obstruction can allow blood to flow back into it. If this occurs, then the tissue will regain a more normal color. If not, then that section of bowel has to be removed, and the cut ends reattached. This is referred to as an resection-anastamosis. If a small section, of bowel is compromised (a few feet), then chances of survival increase. However, if large amounts are affected, prognosis will drop quickly. A horse can have up to 50% of its small intestine removed, but taking 30-40 feet of SI out is a risky endeavor. Many times, the decision needs to be made whether to finish the surgery, or to euthanize while under anesthesia.


If the horse is recovered, the battle doesn’t end once surgery is done. Initial recovery for these horses requires about 2 weeks in a hospital with IV fluids, antibiotics and pain medications. Diets are slowly introduced to allow the gut to heal and not have to work too hard. These horses have to be monitored very closely for secondary signs, such as recurrence of colic or for laminitis.
Small intestinal strangulations are one of the more severe types of colic. Treatment must be fast and aggressive, and even then it’s not always successful. Always have a trailer readily available in case you need to transfer to a surgical facility. Time can be critical in these situations, and an hour can make a huge difference.