Equine Cushing’s disease is a fairly common term in the horse industry. That’s because 1 out of 5 horses over the age of 15 have the disorder. But for how common Cushing’s is in horses, there remains a lot of misunderstanding about this condition. In this blog, we’ll try to make things a little more clear!
Note: While Cushing’s disease can contribute to other metabolic disorders (such as insulin resistance), we’re going to focus solely on Cushing’s disease for the purpose of this post. We’ll tackle insulin resistance in another blog post!
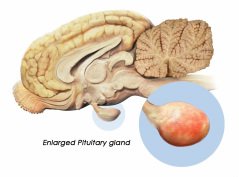
The term Equine Cushing’s Disease was coined for the similarity to the syndrome in humans and dogs. (Cushing’s disease in humans was originally described by a neurosurgeon at Johns Hopkins University named Harvey Cushing.) In humans and dogs, Cushing’s is most commonly caused by either 1) an adrenal tumor or 2) a tumor in the anterior lobe of the pituitary gland which causes hyperplasia (excessive growth) of the adrenal gland. Both of these cause an increase in cortisol (a steroid). In horses, Cushing’s is primarily due to a tumor in the intermediate lobe of the pituitary gland, but there is no associated hyperplasia of the adrenal gland. That’s why the technical name of it is Pituitary Pars Intermedia Dysfunction (PPID). Whew! If you thought that was scientific, just wait!
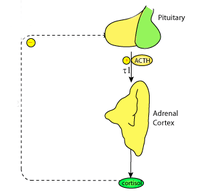
So what exactly is going on to make this disease such a concern? Well, as the pituitary tumor grows, it secretes a hormone called ACTH (Adreno-Cortico-Trophic Hormone. Yes, it’s a mouthful!) This hormone signals the adrenal gland to secrete cortisol, also known as a “stress hormone”. The chronically increased level of steroids in the body wreaks havoc on the balance that the system usually tries to attain. This is what leads to the common signs of PPID.

The most common sign of Cushing’s is excessive hair growth and inability to shed out appropriately (known as hirsutism). This can affect up to 80% of horses with Cushings. Other things we often see are lethargy, weight loss/muscle wasting, recurrent infections (such as hoof abscesses) and chronic laminitis. If we see horses with these signs, we may recommend further testing. However, in some instances, clinical signs are obvious enough, and we will merely recommend to start treatment.
Testing for Cushing’s can be done in a few different ways, but they mainly focus on circulating levels of ACTH. You might say, “Well, if cortisol levels are increasing, why don’t we just test for that?” Glad you asked! In the past, horses with PPID have shown cortisol levels that are either increased, normal or decreased. Cortisol fluctuates throughout the day and from one individual to another, so it is very difficult to make an accurate assessment of any disease process by associating with steroid levels.
So on to the tests we do use! The first (which we typically rely on) is to test the resting ACTH levels. This is simple enough – if the measured level of ACTH is above or below a certain threshold, the horse is positive or negative, respectively. Caution must be used with this as there is a 3-fold increase in the fall, but this has been measured in normal horses, so we can adjust values for that. The second test is known as a Dex Suppression Test, whereby a blood sample is taken, then a small amount of dexamethasone (a steroid) is administered. A second blood sample is taken approximately 20 hours later. This test should cause a significant drop in the amount of ACTH present. If it does not, then the horse is positive for Cushings disease. However, this test can be concerning as we are giving steroids to a horse with possibly high circulating levels of steroids. Since excessive levels of steroids can rarely cause laminitis, we reserve this test for specific cases.
If results of the resting ACTH are not significantly elevated, we can do an additional test to rule the disease in or out. This is called a Thyrotropin Releasing Hormone Stimulation test (TRH Stim for short). This test is similar to the dex suppression test in that a sample is drawn, the TRH is administered, and a second sample is drawn 10 minutes later. Again, we will be looking at ACTH levels and how much they rise after administration of the hormone. This gives us a very reliable test to determine the presence or absence of Cushings disease, without the added risk of giving Dexamethasone to a potentially laminitis-prone animal.

If we have successfully diagnosed Cushings disease, or just suspect it based on clinical signs, treatment includes a combination of medical therapy as well as management. Currently, the only approved drug for Cushing’s Disease is Prascend® (pergolide). This is a daily medication that will need to be given for the remainder of the horse’s life. This drug aims to reduce the amount of circulating ACTH, thereby decreasing cortisol levels. We often see a quick turnaround with horses once we start them on Prascend – owners will often comment that their horse seems to have “dropped 10 years” a month or so after treatment starts.
For a long time, pergolide was only available as a compounded formulation. Now that we have an FDA approved form, we don’t recommend or even dispense the compounded drug. This is because studies have shown that compounded pergolide is not stable and does not have a very long shelf life. The concentration of compounded drugs is also quite questionable and is not always what the label states. Check out this study published in the Journal of the American Veterinary Medical Association on stability of compounded pergolide. In addition, compounded pergolide is no longer allowed under FDA rules.
The other aspect of treating Cushing’s is management. Since Cushing’s disease will often lead to insulin resistance (again, more on that in another blog!), it is usually important to control the intake of starches and sugars in the diet. These horses should obtain most of their calories from low-starch hay and fat (since fat is a much safer form of calories than starch/sugar for horses with metabolic conditions). An appropriate diet should be outlined with your veterinarian for best results. Appropriate foot care is important, to reduce the incidence of hoof abscesses and laminitis. Finally, horses with Cushing’s disease should always be managed more carefully with regards to wounds, parasite control – their immune system is often not 100% normal due to the effects of cortisol, so they will always be prone to chronic infection, non-healing wounds, or higher parasite burdens. Your veterinarian can help you come up with a plan to reduce these risks.
While Cushing’s disease is common and incurable, it can be successfully managed. Through owner and veterinary diligence, we can help keep these horses happy and relatively healthy for many years.